Anlylosing spondylitis
A type of inflammatory arthritis, which primarily affects the back. Young patients(less than 40years) present with low back pain which is worse in the early hours of morning waking him up from bed. It improves as day progresses and also with exercise and NSADS. It is associated with a specific genetic test in the right clinical settings, HLAB27. Inflammation in other joints, eyes and big arteritis of heart could be associated as well. There is also increased association of inflammation in the bowels along with AS. People with AS and bowel symptoms of frequent blood and mucous should be investigated promptly.
There is always a delay in diagnosis of this condition mainly because of non-recognition of symptoms both by patients and medical professionals. Diagnosis is confirmed by raised markers of inflammation in the blood, X ray of SIJ showing inflammation of sacroiliac joint or MRI showing evidence of inflammation in the spine.
Mainstay of treatment is NSAIDS and exercise. Physiotherapy is the main pillar of therapy. Patients will have to maintain exercise regimen life long. Among the DMARD therapy, Sulphasalazine has been effective in spinal disease and tendon pain; Anti- TNF therapy had good results if initiated appropriately.
Despite of treatment some patient will go on to develop fusion in the spine resulting in loss in movement. Work place and home adjustments need to be done accordingly. Driving will need help of extra mirror in case neck is affected. NSAIDS can cause damage to kidney or heart, hence close monitoring is required. People tend to live normal life
Childhood Arthritis
Arthritis in children of less than 16 years of age
According to ILAR- International League Against Arthritis Juvenile idiopathic arthritis (JIA) are of the following types [Length of illness before detection is 6 weeks]
Systemic JIA
Polyarticular JIA, RF-positive
Polyarticular JIA, RF-negative
Oligoarticular JIA
Persistent-It affects 1 to 4 joints.
Extended-Over time it affects 5 or more joints.
Psoriatic arthritis
Enthesis-related arthritis
Other arthritis (This is also called undifferentiated or unclassified arthritis.)
According to ACR- American College Of Rheumatology Juvenile Rheumatoid arthritis (JRA) are of the following types [Length of illness before detection is 6 weeks]
Systemic JRA
Polyarticular JRA. It affects 5 or more joints.
Oligoarticular JRA. It affects 1 to 4 joints.
JRA does not include similar types of childhood arthritis (juvenile ankylosing spondylitis, juvenile psoriatic arthritis).
According to ELAR- European League Against Rheumatism Juvenile chronic arthritis (JCA) are of the following types [Length of illness before detection is 3 weeks]
Systemic JCA
Polyarticular JCA. It affects 5 or more joints and is RF-negative.
Juvenile rheumatoid arthritis. It affects 5 or more joints and is RF-positive.
Oligoarticular JCA. It affects 1 to 4 joints.
Juvenile psoriatic arthritis
Juvenile ankylosing spondylitis
Arthritis in children less than 16 years of age with persistent symptoms more than 6 weeks and no other cause has been found to cause these symptoms. Systemic presentation is more common in 1to 6 years of age. Young girls are more affected with both poly-articular and pauci-articular whilst a particular type of pauci-articular seems to be more common in boys. The polyarticular type with positive Rf carries a worse prognosis compared to Rf negative ones.Joint pains, joint swelling, fevers, and rash are some of the common features. There is prolonged stiffness in the morning. Commonly affected joints are knees and hands although any joint could be affected. Some children may develop lymph node swelling as well. Eye inflammation could also be part of the whole spectrum. All children with arthritis should have their eyes checked. Children growth could be affected as well.
There is no single test that will tell if your child has arthritis or not. Instead it is diagnosed with a combination of symptoms, clinical examination, and blood test, X rays, USS as required. Family history of autoimmune disease imposes increased risk.
Treatment is individualised and support is needed for the child from physical adaptations and psychological point of view. Commonly used medications to relieve symptoms are NSAIDS like Ibuprofen, Naproxen and Steroids are used in various form- oral, intra-articular, IV. DMARD like MTX are used and has been found safe in children. Biologics are also available. Physiotherapy and occupational therapy are required. Exercise is important to maintain function and range of movement of joints.
Fibromyalgia
It is a fairly common condition causing pain everywhere in muscles and tendons. Women are affected more than men. Patients experience widespread muscle pain, tiredness/fatigue or lack of energy, sleep disturbances, headaches, always remains irritable, feeling low or weepy, irritable bowels, forgetful, poor concentration, increased sensitivity to cold, sound, knocks and bumps.
It is possible that chemical changes in the body’s pain pathways causes this symptoms. It is usually triggered by life events, which could be physical or psychological.
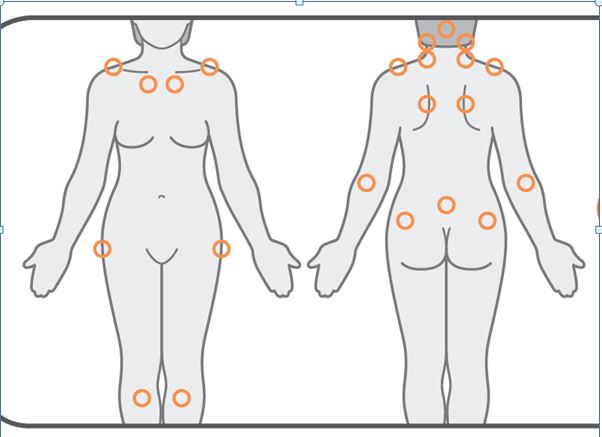
It is mainly diagnosis of exclusion, usually no inflammation or degeneration is found in most cases and it doesn’t cause any structural damage to the body. It means when doctors examine you they only find pain in your muscles and tendons but no swelling is seen, all blood test and x rays and ultrasound scans are normal. People affected are found to have increased sensitivity to pressure or minor knocks that wouldn’t normally be painful. Several factors are taken into account before arriving at the diagnosis apart from normal tests. They are presence of symptoms of more than 3 months, cognitive impairment symptoms like poor memory and concentration, poor sleep patterns, not getting refreshed despite sleeping and having more than 11 tender points out of 20 shown in the image.
Conditions usually found alongside fibromyalgia are chronic fatigue, depression and anxiety, restless leg syndrome – spasms in either or both legs, irritable bowel syndrome (IBS), temporomandibular joint disorder (TMJD) – problems with the joint connecting the jawbone to the skull, hypothyroidism.
Treatment comprises of medication and other forms of therapy. Medications to relive pain and improve stiffness in muscles, improve sleep and physiotherapy. Painkillers like paracetamol and opiates only tend to take the edge of the pain so use it judiciously. Opitaes are addicting and does not provide with lot of lot of benefits so keep them to minimum. Amitriptyline and Dosulepin may improve muscle stiffness and improve sleep, take it few hours before going to bed. It takes few weeks to notice benefit from them. Anti-depressant and neuro pain modulater like pregabalin and gabapentin has also been found helpful. Physiotherapy, Pilates, hydrotherapy, acupuncture can also be helpful.
You can help yourself by having a better understanding of the condition, pacing plays a very important part in managing the symptoms around your daily activities. Exercise like walking, swimming, if you can’t swim simply walk in the swimming pool on the shallow end. Talk to people who have similar condition and share your experience. Eat and drink healthy, stop smoking, avoid food and drink before bedtime. Try to manage anxiety as best as you can. Go out and socialize.
Gout
It is one of the most painful forms of arthritis. Often it starts with severe inflammation of big toe, also known as Podagra. The affected joint is sore to touch, swollen and most of the time associated with redness on the skin mimicking cellulitis. It can affect any joint. It is caused by excessive accumulation of uric acid/urate in body, which is either due to more production or commonly less excretion from the body. These forms mono sodium urate crystal in an around the joints mainly the cartilage and causes intense inflammation when they come of it into the joint cavity.
Men are affected more than women. Gout in women tends to occur after menopause. Excessive alcohol is commonly associated with gout but it is not the only cause. People who are overweight, have excess cholesterol in their body, cannot get rid of the urate produced in the body due dysfunction of kidney, or in whom gout runs in the family are some kwon common factors contributing to gout. In some cases it is due to excessive breakdown of cells in certain blood disorders, rarely it is also inherited as part of some genetic condition.
It is diagnosed with the typical symptoms, if possible then by taking some fluid out of your affected joints to looks for the crystal. X ray can show changes due to gout in late stages. Recently USS has been beneficial to identify crystal in the joint line. Other special scan are available but they are not usually need. Tell tell sign of Gout is a tophi which is basically excessive accumulation of urate crystal, common sites are elbows, ear, fingers. People can also develop kidney stones as results of excessive uric acid.
Treatment is with lifestyle modifications and medication. Most important is life style medication- reduce weight, take healthy and adequate diet which should be monitored for protein, minimum or no alcohol, exercise and adequate fluid intake., stop smoking. In terms of medication, during acute attack NSAIDS along with stomach protection (either with PPI or ranitidine) or colchicine or steroids. Once the acute attack has settled then if you have risk factors like kidney dysfunction or you are on water tablets (diuretics), or you had kidney stones or have tophi, you should be started on Allopurinol. Your doctor would monitor and adjust the dose accordingly. Other option available is Febuxostat.
Never stop Allopurinol or Febuxostat during an acute attack if you are already on it for previous gout. Continue them, alongside take either NSAIDS or colchicine or steroid. If you are unable to tolerate Allopurinol of Febuxostat, there are other drugs available which you doctor can prescribe.
Osteoarthritis
This is by far the commonest form of arthritis seen. It can affect any joint. It causes pain and stiffness but no or minimal inflammation. After having it for a while you might lose movement in that particular joint like end of finger joints (PIP)and develop bony swelling- OA nodes. Occasionally, there is stiffness in the morning but overall symptoms are worse in the evening and night. You can also feel grinding sensation like crepitus in knees.
Commonly affected joints are base of thumb, end of finger joints (PIP and DIP), knees, hip and back and base of big toe(1st MTP). Peri-menopausal women in late forties have increased susceptibility to OA. Positive family history, physically demanding job with repetitive movement, trauma and previous damage to joints due to inflammation often predisposes to develop OA early. Excessive body weight predisposes to knees, hip and spine OA. Diagnosis is from your history and lack of inflammation seen in the joints along with nodes and crepitus. Blood test for inflammation are normal and antibodies for arthritis are negative and X rays shows osteophytes.
Treatment is keeping up the muscle strength with regular exercise; painkillers are used to help with pain. Physiotherapy and swimming helps to regain and maintain muscle strength. Weight reduction plays a crucial role in controlling the progression. Topical anti-inflammatory gel can be used on the affected joints. Capsaicin cream (chilli) is useful on knees. Intra articular joint injections are also helpful in the beginning then gradually lose response. Joint replacement is indicated when above measures fail to control pain, knee and hip replacement has had most success.
Never stop Allopurinol or Febuxostat during an acute attack if you are already on it for previous gout. Continue them, alongside take either NSAIDS or colchicine or steroid. If you are unable to tolerate Allopurinol of Febuxostat, there are other drugs available which you doctor can prescribe.
Osteoporosis
This is a condition that affects bones, your bones are weaker than expected at your age and is at risk of fracture with minimum injury. Osteomalacia is a similar condition but is of less severity and minimum fracture risk. Treatment also differs. Women are at risk, after menopause they lose bone very quickly. This is aggravated by inadequate intake of calcium and vitamin D, lack of exercise, smoking, alcohol, family history of osteoporosis, inflammatory medical conditions like RA, IBD, etc and certain drugs like used breast cancer and prostate cancer. Disease, which affects absorption from gut like coeliac, which affects mobility as it, causes muscle disuse and stagnation in bone remodelling exacerbates bone loss and contributes to it. Early menopause and steroid use for more than 3 months are biggest risk factors.
This can cause silent fractures in your back bones(vertebrae’s), or it can cause fracture and pain. Likely sites are hip, spine and wrist. People with above risk factors, low body mass or history of low trauma fracture should have DEXA scan done and bone health checked.
Diagnosis is based on DEXA scores taking into account of accompanying history. Typically T (bone health when compared with young woman)score of less than 2.5 is classed, as osteoporosis while less than 1 is classes as osteopenia. High Z score (ie bone health compared to person of your age) has increased risk of fractures. Treatment is recommended if you already have 2 or more back bone fracture or hip fracture irrespective of DEXA score or your T score is less than 1.5 and you are on more than 7.5 mg of steroid daily for 3 months.
It is very important to stop smoking, decrease alcohol intake, exercise at least 5 days in a week, and maintain adequate calcium and vitamin D intake. You should be regular calcium and vitamin D supplements. Medication used to prevent bone loss are- Bisphosphonates, Denosumab, HRT, Raloxifen. Bisphosphonates are a group of drugs used orally (alendronate, residronate etc) or IV (zolendronate). Medications to build up bones are- strontium (not recommended in people with heart disease) and teriparetide s/c injections.
PSA
It is a type of inflammatory arthritis associated with a skin condition called psoriasis. People with PSA either have skin psoriasis, most of them will have nail involvement with psoriasis as well or they might have first degree relative who has got skin psoriasis. It affects joints and tendons. This type of arthritis could also affect back. People suffering from PSA also tend to have metabolic syndrome.
Typical symptoms of PSA are- painful swollen joints, which is not usually symmetrical in distribution. Swollen whole fingers or toes (dactyitis), pain in the end of Achilles tendon (enthesitis), sole of feet(planter fasciitis), red/itchy scaly rash, nail pitting, thickening and discoloration. People can also present with new onset low back pain (buttock pain) and stiffness worse in the morning that improves with exercise and NSAIDS.
Diagnosis is based on your symptoms, joints and tendons showing inflammation on examination, skin and nails showing changes as above. Bloods are checked for markers of inflammation and antibodies to exclude other form of arthritis. X rays, USS or MRI could be used to establish the diagnosis further.
Treatment depends of extent of involvement. NSAIDS are used as first line, persistent symptoms of less than tree joints could be controlled with joint injections. If these measures fail then DMARDS are used- Methotrexate, Sulphasalzine, Leflunomide etc. Failing these then biologics are available, anti-TNF have most success in this group other new group of drugs have also become available.Skin psoriasis is treated with ointments, retinoid, and ultraviolet light therapy before DMARDS and biologics are used.Physiotherapy and occupation therapy plays important supporting role in helping with joint pain and maintain mobility and independence.
Rheumatoid Arthritis
An autoimmune inflammatory arthritis, which causes stiffness early in the morning, pain and swelling in the joints. It is a systemic disease as it can affect lungs, eyes, and skin and can also cause inflammation in the blood vessel. Autoimmune diseases occur when our own body defence system (immune system) fails to recognise some part of our system. It results in production of antibodies like rheumatoid factor and CCP, which inters attacks body system causing the disease.
There has been a lot of research into understanding of the disease process and its treatment, which has changed the face of arthritis. It used to be very debilitating and deforming form of arthritis affecting activities of daily living resulting in loss of personal independence and economic cost of person, family and society. With the advent of DMARDS (Disease Modifying Anti-Rheumatic Drugs), a push towards early diagnosis and treatment, we are now achieving to keep people healthy, independent and working.
RA tends to favour women in late forties although it can affect absolutely anybody. There is gradual onset stiffness early in the morning lasting for more than 30 minutes; it gets better as the day progresses. It is not preceded by infection or injury. There is pain and swelling affecting joints- especially affecting knuckles in the hand and base of toes in the feet. Wrist, shoulders, elbows and ankles could also be involved. The joint involvement is symmetrical in nature. Occasionally neck in also involved. Affected joint are very painful resulting in loss of movement as well. It responds very well to NSAIDS- oral or topical. Other system could be involved like eye and the lungs. You might develop nodules in your body. Because of on-going inflammation in the body, sometimes there is flu like symptoms along with sweating, weight loss, loss of appetite leading to tiredness, low mood, anaemia.
Diagnosis is made if you have joint symptoms for at least more than 6 weeks along with blood test showing inflammation and presence of antibodies like rheumatoid arthritis and CCP. X rays are done initially as baseline to compare later on but it does not aid in early diagnosis as X ray changes appear only after disease has done the damage. Ultrasound of joints can pick up early inflammation. MRI scans are very good at showing early inflammation but are costly tools still and not often required to make a diagnosis.
Treatment comprises of medication, physiotherapy, exercise, occupational therapy, surgery. Medications are of various groups. NSAIDS are first line, both oral and topical. Steroids are the quickest acting anti-inflammatories, they are used in various forms. DMARDs are the main stay of treatment. Methotrexate, Sulphasalazine, Hydroxychloroquine , Leflunomide are some of the drugs frequently used. Methotrexate changed the face of rheumatoid arthritis while the biologics had revolutionised the treatment. Biologics are group of drugs, which targets various parts of inflammatory process itself. They are very costly and not without side effects, hence appropriate monitoring is required and should be used by experts who have experience in using it. Biologics currently in use are of various groups- anti-TNF(Infliximab, Etanercept, Adalimumab, Certolizumab, Golimumab), Rituximab, Tocilizumab, Abatacept. Tofacinitib is another new drug available.
In order to protect your joints it very important to follow advise from physiotherapist and occupational therapist as it helps to manage the long-term outcome of your condition. Sometimes surgery becomes inevitable to help counter the joint problem when above has failed especially with large joints. Surgeons also play important part in cases where tendon repairs are required.