Types of Haemorrhagic Stroke
These are bleedings in the superficial areas of the brain. They are near the skull bone and by definition should be within 2 cm depth from the skull bone. From a surgical point of view they are easier to access for operation and removal if necessary. Bleedings due to amyloid angiopathy, aneurysms and arteriovenous malformations are generally superficial or lobar.
These bleedings are deep into the brain tissue and are not accessible for surgery. Bleedings due to high blood pressure are typically in deep locations.
Hypertension (high blood pressure): High blood pressure is by far the commonest cause of bleeding in the brain. In the Indian population due to lack of any public health screening programme high blood pressure often remains undiagnosed and unknown to patient. Lack of treatment results in uncontrolled high blood pressure resulting in a far high percentage of haemorrhagic strokes in Indian population. Equally on the other hand this is a treatable condition. Early recognition and treatment of high blood pressure can result in reducing this fatal kind of stroke in our population.
Amyloid Angiopathy: With age an abnormal protein called amyloid gets deposited in the walls of the blood vessels of brain. This alters the character of the blood vessel wall and can make it more prone to leak and rupture. This can result in increased risk of bleeding in the brain. The cause and risk factors for this disorder is still not understood in detail. Age, smoking, high blood pressure are thought to be related to this disorder. Diagnosis is possible with MRI imaging. There is no treatment available at this point other than avoidance of any blood thinning medication like aspirin, Clopidogrel or warfarin. In very selected and few cases steroids may be beneficial.
Arterial aneurysm: Aneurysms are weak areas of blood vessels. These can be found in any area of the body including the brain. The wall of the blood vessel in an aneurysm is weak and therefore the blood vessel expands from the pressure of the flowing blood forming a sac like structure. These sac like structures with weak blood vessel walls do not cause any symptoms but are at high risk of rupture and cause bleeding into the brain.
Arteriovenous malformation: These are an abnormality of blood vessels where different kinds and sizes of blood vessels form a network within the brain. The blood flow through this net of blood vessels is abnormal and is at risk of rupture and bleeding into the brain.
Cavernomas: These are very small blood filled spaces within the brain which can rupture and bleed from time to time.
Tumours: Tumours of the brain (whether arising in the brain or spread from another tumour elsewhere in the body) have a tendency to bleed inside them.
Coagulation disorders (disorders of blood clotting): Various diseases of blood and liver can cause abnormality of clotting of the blood which can increase the risk of bleeding anywhere in the body including the brain.
Viral infections: Certain viral infections including Hepatitis B, Hepatitis C and HIV (AIDS) can cause increased risk of bleeding in the brain.
Symptoms of Haemorrhagic Stroke
Recognising stroke early is of paramount importance as there is only a short time window where the treatment is effective and brain damage can be reversed. To provide advanced medical interventions in a timely manner a stroke needs to be recognised early across the board, by patients, their family members and medical professionals
The person who is having the stroke may not recognise what is happening to him as his brain is not working. Therefore it is useful for all to have an awareness of symptoms of stroke so that people around the victim can recognise the problem and ask for help early. This necessitates development of simple and easy to use assessment tools to be used by Non Stroke specialist doctors, Allied health professionals and bystanders to recognise Stroke. Awareness programmes play a vital role to make the general population aware of the importance of recognising stroke early and how to use the assessment tools to do so
A few assessment tools which are in common practice in the developed countries has been decribed below
 The FAST tool has been developed and is commonly used in the United Kingdom. It is an assessment tool for use of lay persons and bystanders to quickly recognise Stroke and urgently seek medical help. Significant efforts have been made in recent years to spread the awareness about this tool among general population including widespread campaign through public media. The tool involves quick assessment of facial asymmetry, power of arms and speech of patient within the ability of a layperson as described below.
The FAST tool has been developed and is commonly used in the United Kingdom. It is an assessment tool for use of lay persons and bystanders to quickly recognise Stroke and urgently seek medical help. Significant efforts have been made in recent years to spread the awareness about this tool among general population including widespread campaign through public media. The tool involves quick assessment of facial asymmetry, power of arms and speech of patient within the ability of a layperson as described below.

Ask patient to show teeth, Is there an unequal smile or grimace
Note which side does not move wellLift the patient’s arms together to 90º if sitting, 45º if supine and ask them to hold the position for 5 seconds before letting go, does one arm drift down or fall rapidly?
If one arm drifts down or falls, note whether it is the patient’s left or right.Listen for NEW disturbance of speech, or slurred speech.Listen for word-finding difficulties with hesitations.
Asking the patient to name common objects like a cup, key or watch.IS THIS NORMAL FOR THEMIt's TIME to ring an emergency ambulance
The FAST tool have become very popular in recent years and work as an effective means of recognising stroke early and getting immediate medical attention Click here to watch a relevant video(THE FAST TEST)
ROSIER: The Rosier tool which stands short for Recognition of Stroke in Emergency Room was developed to help early recognition of stroke in the Emergency Department by Non Stroke specialist doctors. There are of course a number of conditions which may mimic stroke at the onset and make diagnosis difficult for non specialists. The ROSIER is specifically aimed to help to differentiate these Stroke mimics from an Acute Stroke.
Click here to download a sample Rosier Scoring System document
CT Brain scan: This scan is nearly 100% sensitive for a bleeding in the brain and is extremely useful to do immediately on presentation of the patient.
Vascular (blood vessel) imaging: This is done either by a CT angiogram or MR angiogram. Both are sensitive to variable extent for detecting aneurysms and arteriovenous malformations.
MRI Brain: This is sensitive to detect underlying abnormalities of brain structure that may have caused the bleeding. They are particularly sensitive to detect brain tumours and arteriovenous malformations.
Digital Angiogram (DSA): This is an actual angiogram done in the same way a heart angiogram is done. A doctor will introduce a catheter or tube into the blood vessel through the groin or wrist. The tube is then migrated to the blood vessels of the brain where it injects a dye. Real time pictures are then taken with this dye showing up the blood vessels of brain in great detail. If the suspicion of aneurysm or arteriovenous malformation is high, but CT or MR angiogram is not showing any abnormality, a DSA can be considered. It is more sensitive than the CT or MR angiogram to pick up micro aneurysms or micro arteriovenous aneurysms.
Blood tests: Routine blood tests looking at blood count and clotting tests of blood should be performed. In addition liver blood tests, kidney blood tests and tests for Hepatitis B & C and HIV should be considered.
Blood pressure control: Emergency blood pressure control is extremely important after bleeding in the brain. Reducing blood pressure quickly after haemorrhagic stroke within 6 hours of onset of symptoms has been shown to reduce disability in future.
Clot stabilising drug: It has been shown that clot stabilising drug called Tranexamic acid helps to stop or reduce the amount of bleeding in the brain if given urgently after haemorrhagic stroke, preferably again within 6 hours. It is still thw subject of research whether such reduction of bleeding translates in improved survival and disability after stroke.
Surgical removal of blood clot: Several medical research studies have shown that routine surgery to remove the blood clot from brain does not result in better survival and does not improve disabilities. It si currently therefore not a routine procedure after haemorrhagic stroke. It is offered to selected patients in whom the blood clot is large and causing pressure on other brain structures which can be life threatening.
Clotting products: There are several clotting products available in market from Fresh Frozen Plasma to Prothrombin complex concentrate. These are various blood products with different combinations of clotting factors in them. They can be useful in controlling brain bleedings if they have been caused by use or overuse of blood thinning medication like warfarin.
ICP Bolt: This is similar to a screw which is drilled into the brain through the skull and continuously monitors the pressure inside the brain. It is particularly useful for patients who are unconscious or anaesthetised after a haemorrhagic stroke. Any increase of pressure inside the brain may indicate increasing bleeding in the brain that may need surgery.
Aneurysm surgery: If the brain bleeding is caused by a rupture of an aneurysm, various kinds of emergency procedures can be performed to stop bleeding. These can be done by open surgery or access through the blood vessel like an angiogram. Different techniques employed are coiling or clipping the aneurysm to arrest bleeding.
Blood clot aspiration and drain: It is believed that strict control of blood glucose after the immediate aftermath of stroke is beneficial to limit brain damage. This is done by infusing a drip of insulin through the veins with hourly checks on blood glucoseThis technique is still under research but is showing some early promise. A neurosurgeon under guidance from CT or MR introduces a needle into the blood clot inside the brain and aspirates as much as possible. A drain is left inside the blood clot for next 2-3 days to allow further drainage of any loose blood clots outside the brain. Occasionally blood thinning or clot breaking drugs can be administered through the drain to break the clot and allow it to drain outside easily.
External Ventricular drain (EVD): Under normal circumstances a type of fluid called Cerebrospinal fluid (CSF) circulates through channels within the brain and the spaces around the brain. Either the bleeding in brain itself or pressure from the bleeding may block the circulation and drainage of this fluid. This leads to increased pressure from undrained CSF in the channels of brain causing a life threatening condition called Hydrocephalus. Diagnosis is made by doing CT scan of brain. This can be prevented or treated by putting a drain from outside through the nose in the channels of the brain, thus helping the blocked CSF to drain outside. This is called external ventricular drain or EVD and its insertion can be a life saving intervention.
Blood pressure control: Just like in the emergency setting blood pressure control over longer time remains the most important measure to treat haemorrhagic stroke and prevent recurrence.
Aneurysm surgery: Aneurysm surgery if not done immediately can be taken electively at a later date.
Stereotactic radiosugery: This is a form of laser treatment used to treat small to moderate sized arteriovenous malformations or cavernomas. Laser is directed accurately with CT or MR guidance to the area of arteriovenous malformation or the cavernoma which then obliterates the lesion.
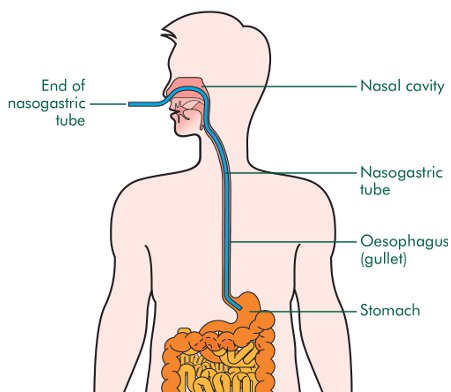
Feeding: All stroke patients should receive dietician input to establish a feeding regime. Nutrition after stroke is extremely important to maintain muscle bulk and power and therefore has a positive influence on rehabilitation outcome. If the swallowing assessment shows that the patient is not able to swallow safely then alternate methods of feeding should be implemented urgently. A nasogastric tube should be used in the immediate period after stroke. This is a tube passed through nose into the stomach through which food can be passed without the patient swallowing. If after 4 weeks the swallowing is still deemed to be unsafe a PEG (gastrostomy) tube should be considered. This involves passing a tube directly into the stomach of the patient through a hole on the skin above the stomach. This can be used as a more permanent method of feeding the patient.
Video credit attributed to: http://pocketsnips.org
Picture credit attributed to: https://en.wikipedia.org/wiki/Nasogastric_intubation

Picture credit attributed to :http://www.oralcancerfoundation.org/

Rehabilitation: The scope of this topic is large and we are only going to touch on this currently. The natural history o Ischaemic stroke will suggest that the disability will be most at onset and then improve from thereon. The most improvement is in the 1st two weeks, followed by continuous improvement for next 3 months. Most patients will plateau after this, but some continue to improve up to a year after stroke. Early mobilisation and rehabilitation is paramount to reduce disability after stroke. This is a multidisciplinary approach involving physiotherapists, occupational therapists, speech therapists, swallowing specialists and of course the stroke doctor. Various exercises are directed at improving muscle power and balance by physiotherapists while occupational therapists work with more complex tasks like dressing one self. Mental exercises are also used to improve brain functioning in various fields. Loss of speech is a common symptom after stroke and the speech therapists teach various techniques for the brain to overcome or work round these problems. It is recommended that able patients receive 45 minutes of rehabilitation from each of these specialists every day.
In essence, parts of the body have to re-learn the vary basic activities like moving, swallowing, speaking etc following a stroke and it is only achievable with help from well trained and specialist team of physiotherapists, occupational therapists and speech therapists.
Post stroke pneumonia:
Pneumonia or severe chest infection is one of the commonest complications after stroke. Often after stroke the muscles inside the mouth used for swallowing are paralysed, as well as the muscles used for coughing. This results in food, drinks and patients own saliva going down the air pipe into the lungs causing pneumonia. Between 20 – 30% of patients with stroke will develop a chest infection of some sort. This is a dreaded complication which increases the chances of death significantly post stroke. Patients with large strokes who have lost swallowing function are at particular risk. Immediate assessment of swallowing function post stroke is the most important step to prevent post stroke pneumonia. If the test suggests problem with swallowing then the patient should not be allowed to eat or drink normally, but should be fed through a tube inserted through nose or mouth.
Post stroke pneumonia is diagnosed with help of clinical examination, chest x-ray, blood tests. It should be treated aggressively with antibiotics through the drip into the veins.
Hydrocephalus: Under normal circumstances a type of fluid called Cerebrospinal fluid (CSF) circulates through channels within the brain and the spaces around the brain. Either the bleeding in brain itself or pressure from the bleeding may block the circulation and drainage of this fluid. This leads to increased pressure from undrained CSF in the channels of brain causing a life threatening condition called Hydrocephalus. Diagnosis is made by doing CT scan of brain. This can be prevented or treated by putting a drain from outside through the nose in the channels of the brain, thus helping the blocked CSF to drain outside. This is called external ventricular drain or EVD and its insertion can be a life saving intervention.
Clotting in Leg (Deep vein thrombosis): In a normal scenario when a person walks or moves the muscles of leg and calf contracts and this helps to get the blood flow back to the heart. Often patients after stroke, especially ones who have suffered a large stroke, are kept immobile in bed. This results in blood pooling and being stagnant in their legs with compromised blood flow. As a result often blood clots in their leg causing deep vein thrombosis (DVT). The symptoms are swelling, redness and pain in leg. Early mobilisation after a stroke is paramount in preventing clot formation in leg. Recently use of electronic devices (IPC or Flotron boots) which makes the calf muscles contract periodically when the patient is at rest has been shown to reduce these complications. It is treated with medication like warfarin or heparin (anticoagulation) to thin the blood and not allow it to clot further. The duration of treatment is usually between 3 to 6 months.
Clotting in Lung (Pulmonary embolism): The mechanism of developing this complication post stroke is similar to formation of clots in leg. Due to relative immobilisation of the patient post stroke, clots form in leg and can then migrate with blood flow directly to lung. Clot in lung (Pulmonary embolism) though is a much more serious and life threatening complication than clot in leg (DVT). Measures to prevent are similar to above in early and active mobilisation post stroke, use of electronic devices (IPC or Flotron boots). If confirmed this should be treated immediately with medication that prevents further clot formation like warfarin or heparin (anticoagulation). In special circumstances a device like an umbrella is placed in the blood vessel between the leg and lung to prevent migration of clots from leg to lung. The device is placed in a blood vessel called Inferior vena cava (IVC) and is therefore called IVC filter. It is placed under radiological guidance through a small cut in the groin. It is usually a straightforward procedure with very few complications. The device may be taken out later if needed.
Post stroke seizures:
Seizures or fits (similar to attacks in patients with epilepsy) are an extremely common complication after stroke. It is relatively uncommon to occur at the onset for Ischaemic stroke, but may occur anytime afterwards from the first week to 20 years afterwards. Common symptoms may range from violent shaking of all arms and legs, to twitching or rhythmical shaking of a particular arm or leg or simply vacant looks and being unresponsive for some time. Patients may be drowsy or irritable after an event and often complain of a headache.
It is generally diagnosed from accounts of events given by patient’s relatives or other witnesses to the events. An EEG (study of electric waves in brain; generally done by putting electrodes on the head and studying the electric impulses) is often done but gives limited information towards a diagnosis. It is treated with antiepileptic medications which prevent seizures. Common medications used are Sodium Valproate, Levetiracetam (Keppra) and lamotrigine.
Post stroke spasticity (muscle stiffness): After stroke often muscles develop severe stiffness due to long term remaining paralysed and unused. Usual symptoms are pain in muscles and difficulty and resistance in moving joints. This can be treated with muscle relaxant medication initially. On occasions this is treated with an injection of muscle relaxant (Botulinum toxin, BOTOX) directly into the muscle.